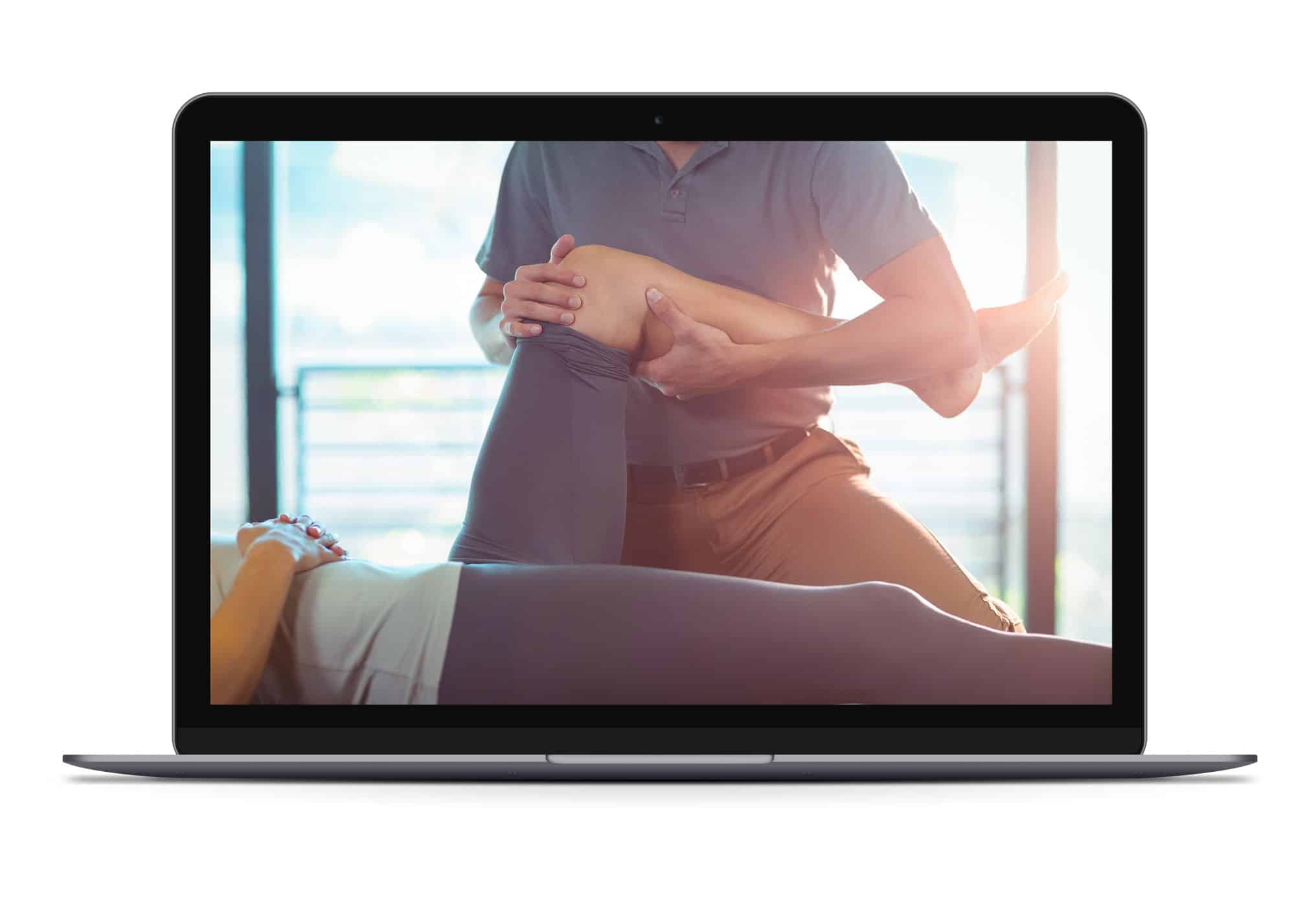
As a physical therapist, nothing’s worse than seeing a runner who has lost confidence and trust in their body. Luckily, I know how to get runners back on track. Using my 20+ years of experience, I’ve outlined the 8 most important strategies to keep in mind when working with runners who seek your guidance and help in the face of a setback.
1 – Leveraging “Non-specific Effects” & Refining the Runner’s Journey

It’s important to appreciate that a lot goes into a physical therapy session beyond the specific intervention(s). Believe it or not, the context of an experience (AKA “non-specific effects”) is responsible for more than 4x the variance in treatment outcomes in medicine and rehab.
When you think about the last time you went out to dinner…
- How easy was it to make a reservation, and did you receive a confirmation?
- When you arrived, were you greeted by a friendly host or hostess and promptly seated at your table, or did you have to wait?
- Was the table clean and comfortable?
- Was the server upbeat and warm in their demeanor and patient with you while anticipating your needs?
- Was the food brought out in the appropriate order on time and warm like it just came out of the oven?
- Was the waiter delayed in bringing you the check, and did they accept all payment options?
- Did they thank you for dining with them and mention they look forward to seeing you again soon?
As you can see, a lot goes into a good dining experience beyond the actual food. The same goes for every physical therapy session I have with a runner. By taking the time to understand the factors at play, you can leverage certain effects to improve buy-in, eliminate potential friction, enhance outcomes, and give runners ownership of their situation.
2 – “Inductive Foraging” & Asking Open-Ended Questions

“You can run all the wisdom of science and technical knowledge past an athlete, but behind that sits their heart, values, motivation, and doubt.”
-Stephen Rollnick
When first connecting with clients, create the time and space for them to share their story while posing calculated open-ended questions to help them reflect on their situation.
Did you know that the average time before a physician interrupts a patient is typically 11-23 seconds? Additionally, consults are often rushed, and clinicians can often come across as abrupt, distracted, or sterile.
I can’t help but think back to an experience I had with an orthopedist about a knee injury. After patiently waiting 45 minutes past my scheduled appointment, I finally saw the doc, who seemed to be in a hurry. He spent less than 30 seconds asking me about my knee before quickly examining it and telling me nothing was wrong and that I should “put some holy water on it.” Can’t make this s#*% up.
As much as I want to get to the clinical examination and testing of a consult, I learned early in my career never to rush that initial conversation because it helps build rapport and open communication. Listening to patient stories, connecting, and approaching care through shared decision-making improves my clinical reasoning. This is why my PT consults are 75-90 min long and sometimes longer, pending the situation and needs of the runner.
Below are some powerful questions I routinely incorporate into my physical therapy sessions that I thought would be helpful to mention. The more I can get people to talk openly and honestly about their situation while remaining present, engaged, and genuinely curious, the better.
- Would you mind telling me about yourself and what brings you in today?
- Why do you think you’re in this situation, and why seek help now?
- What steps are necessary to move forward from this point?
- What obstacles might hinder your progress in overcoming this situation?
- Who is part of your support system as you address this issue?
- What is your vision for the coming weeks and months? How do you see things unfolding?
- If I turned out to be the most helpful PT for you, how would your life change due to our work together?
- What would you like to walk out of today’s session with?
- Is there anything else you’d like me to know about you to put me in the best possible position to help you?
Asking these questions invariably garners trust and connection while paving the way to a meaningful and successful outcome.
3 – What’s Point A?
As the great teacher and legendary strength coach, Dan John likes to ask, “What’s Point A?”
As much as we want to rush to “point Z,” which means healthy and consistent training for most runners and perhaps running with reckless abandonment for others, clinicians often fail to clearly identify “point A” during the initial consultation.
Running has predictable performance demands – it also involves relatively high loads performed repetitively over long durations. This is why completing a comprehensive evaluation is imperative for identifying point A.
Want a copy of my Physical Performance Tests & Clearance Considerations sheet I use as part of my comprehensive evaluation? Enter your e-mail below.
Otherwise, you risk giving a runner the greenlight only to have them report hobbling home during their first attempt. It also helps determine whether a runner is a candidate for PT or needs to be referred to a more appropriate provider.
Another benefit is that the assessments can help you develop a bond of mutual respect and trust. Plus, when the approach is collaborative, patients feel acknowledged and optimistic about their abilities. Remember, this objective portion of an assessment is to show runners what they can do more than what they can’t. Just as much as I’m making a mental note of specific impairments or deficits, I’m verbalizing and highlighting a lot of the things that bode well for them.
Finally, it’s also important to watch runners run. Although you’re probably thinking, “DUH,” you’d be surprised how often medical professionals fail to do some form of running gait assessment.
By the time we wrap up this part of the consultation, I have a clear sense of where a runner is on the injury-to-performance spectrum as well as the best next steps to position them for a safe and timely return to training and competition. My primary responsibility from here is to communicate the findings clearly and concisely so they have a refined understanding of their situation and the best next steps.
4 – Load the Tissue with the Issue & The Prisoner’s Dilemma

I consult a lot of runners who are spinning their wheels or can’t seem to get on the other side of a finicky running-related injury. A common denominator in nearly all these cases is failure to load the tissue with the issue.
This is why when crafting a home exercise program for runners, I developed “The L’s of Loading.” It’s ideal for runners with limited time and resources who would benefit from having a simple and actionable home program. Think of it as the 20% of Pareto’s principle.
Below I’ve broken down the L’s of Loading.
- Load the tissue with the issue – often in the form of isolated single-joint exercises
- Life movement – push, pull, hinge, squat, carry
- Linkage exercise – a drill that challenges the kinetic chain.
For example, suppose a runner is recovering from Achilles tendinopathy, and their symptoms have stabilized. In that case, a simple program that might be appropriate based on The L’s of Loading is as follows:
- Load the tissue with the issue ➡️ Single-leg calf raise
- Life movement ➡️ Farmer march
- Linkage exercise ➡️ Step-up
Ironically, after I challenge runners to directly load the tissue or region that’s been bothering them, they often remark, “Is it weird that things feel better after doing the exercise?” Nothing like having a runner discover their pain is malleable as it elicits buy-in and confidence in the program.
Except for certain situations or precautions (i.e., stress fracture), generally aim to “Load the Tissue with the Issue” because taking an avoidance strategy typically doesn’t work.
To read more about The L’s of Loading, you can download the PDF by entering your email below.
5 – Reframing – Highlighting Strengths & Mitigating Threats

“The mentality distracting habit of always looking for faults is so powerful that this shift to focusing on strengths take some getting used to.”
-Jonathan Fader
Most physical therapists and medical professionals are trained in an impairment-based model that emphasizes a runner’s weaknesses or deficits. This approach can often stoke anxiety and have the runner walk out of the session with their tail between their legs.
Rather than rattling off a laundry list of deficits, focus on what’s going well for the runner. For example, I recently consulted a trail runner who came in complaining of right kneecap pain after connecting with a new coach in March who had him running more volume and ‘vert.’ There was no specific event or incident that caused his knee pain. Rather, it was a gradual onset, likely aggravated by long back-to-back runs in the mountains. Despite having some stiffness in his foot and ankle region and being a bit wobbly on that side when performing a lateral step-down, he had several things working in his favor. So I said…
“Based on the lens that I got into your situation and our work today, you have so many good things going for you…
- You’re getting zero pushback during the day with routine activities of daily living (ADLs).
- There’s nothing wrong with your knee joint as full, pain-free ROM and no swelling in or around the joint.
- You can run, hop, and squat on your right leg with no reluctance. Sure, you had some low-level pain though it wasn’t getting worse, nor did it cause you to alter your mechanics.
- Simply bumping up your cadence during the treadmill run also took away nearly all your pain, showing you that nothing sinister is at play.
- If I were in your shoes, I’d carry on but be sensible. I suggest having you run every other day on level ground to rolling terrain for the next couple of weeks. As you prove tolerance to the training, we can start nudging.”
Strive to reframe feedback and data for runners in a positive light while being transparent about the reality of their situation because nothing’s worse than being given false hope.
6 – Communication Heals

“All I did was identify with the patient and give a few encouraging words. It wasn’t anything specific, but I knew it made a difference.
-Austin Smith
If there’s one thing I’ve learned in my 20+ years as a physical therapist and coach, it’s that empathetic communication heals. Taking the time to listen and engage with runners in a curious and non-judgmental manner is the cornerstone of effective care.
Not only is it critical to be present, but word choice, language, tone, explanations, metaphors, and stories convey critical messages and can infuse optimism or sow doubt.
My primary goal with runners is to ensure they feel heard while shifting their attention away from pain, fears, and anxieties and toward healing and recovery. At the same time, I am realistic and transparent about their situation. My aim is to inoculate any unhelpful narratives or thought viruses they may have about themselves and their situation while reminding them of their body’s remarkable affinity to adapt and overcome so long as we create the right ecosystem, respect biology, and appreciate the role of allostatic load.
Just as much as runners come to me for help, it’s also essential to put it back on them. They are the ones who have run into trouble and likely have the best insight as to why. As I always tell runners, “You’re the expert on you, so I’d love to get your thoughts.”
Something as simple as the phrasing of a question regarding whether or not they did their home exercises could make a world of difference.
For example, rather than asking, “Did you do the exercises I gave you?” Try framing the question as, “How have the exercises been going?”
If you work with runners in any capacity, I challenge you to listen carefully while being surgical with your words, stories, and explanations. And remember to put it back on them by asking, “What do you think?”
And never forget, as the great Louis Gifford said,
“Reassurance is a bloody good painkiller.”
7 – Guardrails & The RTF Rule

“Runners don’t have unrealistic goals; they have unrealistic timelines.”
-Curb Ivanic
One of the most challenging and critical aspects of my clinical work is helping runners protect themselves from themselves.
Trust me when I say that left to their own devices, runners often make bad decisions and invariably violate The RTF Rule…Rush to Failure.
This is particularly true in working with runners dealing with bone stress injuries (BSIs), commonly known as stress fractures.
For anyone who’s dealt with a BSI you can probably attest to the fact that once you remove running from the equation, things calm down quickly, and within a matter of a few days or weeks, you’ll think that because you’re pain-free, you’re good to plug back into training where you left off. WRONG. I can think of countless occasions in recent years where runners discontinued the plan of care because they had to get back to training for a big race or to ensure they were ready for the upcoming season. Not only did their plans not pan out, but many of them went on to develop a second BSI. While we’re on the topic and to better understand how bones heal and realistic timelines to return to running as a function of stress fracture locations, check out my buddy Nathan’s posts HERE & HERE.
As much as we hate to admit it, biological healing takes time, and there’s no magic potion or elixir to expedite the process despite what’s presented in the media.
So revel in the process and understand that biological tissue and processes take time. A good rule of thumb is that however long you think it’ll take to get you back to training, multiply it by a factor of 2. And as you plug back into training, an excellent acronym to help progress your running is F.D.D.I. – Frequency, Duration, Density, Intensity. For example, an early goal is to get runners back to running every other day at conversation pace. From there, we can start nudging their runs until they work up to one hour of continuous running. A sensible way to progress things is to incorporate back-to-back running days. And finally, so long as a runner isn’t experiencing any pushback, it is appropriate to layer in some short bouts of intensity in the form of strides or intervals or incorporate some hill work into the equation.
Lastly, I always make it a point to normalize that you’ll feel sluggish and sore as you resume running, especially if you’ve had a more extended layoff. So be patient and forgiving with yourself, and know you’ll be back to full force in due time.
8 – Mapping Out & Signing Off on the Plan

Diligent follow-up and follow-through will set you apart from the crowd and communicate excellence.
-John Maxwell
At the end of every consultation, I make it a point to summarize the session and outline my suggestions regarding the best next steps.
I also make sure to get the runner’s seal of approval by having them verbally agree or sign off on the plan because it’s up to them to take ownership of their situation, and it’s critical that we’re on the same page.
Before parting ways, I also allow runners to voice any questions or concerns that may not have been addressed during the session that they feel are critical to helping them move forward.
Following the appointment, I then email them a detailed roadmap that outlines what they should do over the next three to four weeks in terms of exercises and training-related modifications while again reminding and highlighting the things they have working in their favor and how we’ll segue them from their current status back to running in the manner they’re capable.
In this email, I also include private video hyperlinks to the exercises and any equipment they need to perform their home program. Considering the volatility around certain RRIs, this email must be crystal clear while also providing some autonomy in the way of decision-making for the runner. For example, I often say here are the exercises I want you to do. The order is not critical so long as you get them done, so feel free to plug and play as you see fit.
Another helpful thing is to map everything out on a big whiteboard during the session so runners can appreciate the various moving parts. They can also take a picture of the board as a reference they can always return to. So between that and the follow-up email, they should have a clear path outlined.
CLICK HERE to access this template I created to help you summarize your findings and outline a plan moving forward.
Thanks for taking the time to read this, and hope it helps improve your outcomes in working with runners. If you’re a runner spinning your wheels and want to connect, please reach out HERE, and I’ll gladly help you or get you connected with the right person if you live outside of Seattle.